Sent today first class (as dated, see below)
_____
(own address)
Leicestershire Partnership NHS Trust
Customer Services Team - Complaints
Lakeside House
4 Smith Way
Grove Park
Enderby
Leicester
LE19 1SX
14th August 2014
Dear Sir / Madam
Re. Formal Complaint against Ms.N__ W___ of the Liaison & Diversion Team for failing to safeguard a mentally unwell person, namely J_ ( address removed ).
I am writing this to complain specifically about the conduct of your employee, NW who, in her role as a mental health worker with the new Liaison & Diversion Team, met with my partner, J_ (dob _) on Friday, 18th of July, at Loughborough Police Station.
For several days prior to this, J had been talking about ending her life. She had only just left the Bradgate MH Unit on the 2nd July after an 8 month stay (including a Section 3 MHA order). Her recovery was not absolute, but ourselves and the consultant were eager for her to start a life again at home.
J has a very specific plan of suicide which involves going to the motorway bridge at Junction 23 with the intention of throwing herself off into oncoming traffic. She was starting to express a desire to do this on a daily basis. By Thursday 18th July things became critical again, and having worked in mental health drop-ins myself, I prompted her to follow instructions in her Care Plan. Firstly, she contacted the CMHT and talked to a duty CPN, who, due to the lateness in the working day (4-5pm), told her to contact her GP or the GP-out-of-hours service, failing that, to go to the Urgent Care Centre (Epinal Way, Loughborough). She rang the receptionists at her GP surgery, who could only offer her appointment for the following week. There seemed to be some confusion over what they could do.
We then caught a taxi to the Urgent Care Centre. All the while, J was not sure what to expect and just wanted to leave my side to go to kill herself. We saw two nurses who explained that we would have to go to A&E in Leicester to see the City Crisis Team. J was distraught and left the Urgent Care Centre, and she was running towards the road. As I left to follow, the nurses told us that they would be calling the police. Much further along the dual-carriage way (Epinal Way), J was trying to get to a bus to get to the motorway.
Eventually a police car catches up with us and takes us back to Loughborough Police Station, where we wait in a police car until the Liaison & Diversion team arrive. The mental health worker who saw us then was called V_ (I forget her surname). After a long, practical, yet sympathetic, chat, she told us to wait for a day whilst she faxed and phoned the community team (at Town Hall Chambers, Loughborough) for extra support for J. This gave J something to hold on to, but she was still wanting to end her life. The police then gave us a lift back to J’s house. Still worried about J, I stayed the night.
The following morning I had to leave her briefly, to call at my own house, which is just around the corner from her’s. By the time I returned she was dressed and preparing to leave for the motorway again. I must stress that at no point was J trying to gain access to hospital or asking for special treatment, all she kept telling me was that she wanted “to be dead”. She keeps telling me this. She locks the house door to slow me down. I follow her outside, trying to negotiate with her to come back to the house. Whilst still with her, I called the police. J boards the number 127 bus and buys a ticket to a stop near the motorway bridge, I joined her on the bus, with the police on the phone. I pass the phone to the driver and he is asked by the police to stop the bus. Then the police arrive.
Off the bus, J tries to run away from the police, but we corner her and get her to sit in a bus stop. The police take us back to Loughborough Police Station. J is weeping and apologetic, the whole experience is clearly harrowing. After another a long wait, the L&D Team arrive. This time the mental health worker is NW.
Ms.NW appears to have known J from the past, from when she was working with the County Crisis Team. Her generalisations about J’s lifestyle are based on a woman that I do not know. J is asked if she still sings and why doesn’t “she go back to church?” J currently does neither activities, the last time J did these things was over 12 years ago. NW was very patronising in her manner. Even her way of addressing me with an aggressive “And you are …?” I did not find welcoming.
She described J as having a “robust” care plan with the CMHT and inferred that she should be grateful for an appointment at the end of following week with an OT for an assessment. At this time we were not aware of the appointment since the letter had yet to be received, but events of the following week seemed irrelevant considering the fact that J was in crisis in that very moment.
I remember at one point NW told J “not to be so negative” which I found to be astonishingly dismissive of her problems. She recommended that J went home “…have a cup of tea and something nice to eat, which will make you feel better”, seemingly unaware of her 27 years of eating disorder history (firstly anorexia, then bulimia -J was treated for 10 years at the Leicestershire Specialist Eating Disorder Service which should be in her file), This would have been triggering and alienating to a person in J’s state of mind. NW seemed to be trying to negotiate a little with J, but it mostly comes out as dismissive platitudes, along with something about “choices” as though J was in full control herself. There is no talk of any help or assistance being provided today.
Ms.NW also tells J that if she attempts to go to the motorway again that she “will be arrested for wasting police time”. This upsets J greatly. She regularly suffers from intense feelings of guilt, as part of her anxiety, this makes it worse for her. J is clearly frightened of being arrested, and for the first time mentions that she will “take an overdose”. NW explains that they can give us a lift back to J’s house. J again, says that if she goes home that she will take an overdose with the intention of killing herself.
J determined and frantic, then leaves the foyer where we were talking. The L&D policeman (who gets my name wrong) says that they will catch up with us. I am trying to reason with J. J doesn’t feel that they understand her. The L&D van pulls up and they ask us to get into the back. We comply and they drive us to J’s house. J mentions again that she plans to take an overdose with her prescription medication, of which she has plenty. We are dropped off and left on the pavement near her house.
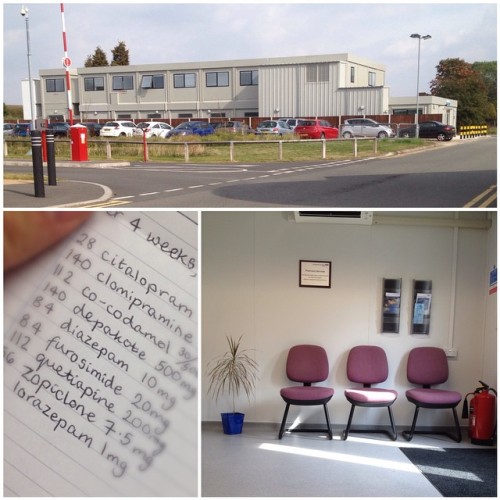
J is still pretty upset at the thought that she could be arrested by police. Back inside her house, I go to get her a drink of water and she starts taking handfuls of pills from packets in a drawer where she keeps her medication. I physically fight with her, trying to stop her taking the pills. I call the police. We struggle, she keeps swallowing pills. Eventually the police arrive, as does a paramedic who later calls for an ambulance. Before we get into the ambulance we count the blister packs and empty packets, J has taken over 120 pills – some of which are very powerful drugs. She is woozy and later passes in and out of consciousness. She is rushed by ambulance to LRI A&E taken straight through into the Resuscitation Dept. She is flushed through for hours with drips and given a special formulae which fights one of the pills (cannulas, a catheter, monitors are used, she is wearing an oxygen face-mask and slapped by a nurse to wake up, it was fairly distressing to see, and that was only after I was finally allowed in). She spends the night in the LRI wired up to monitoring machines and is on oxygen. I stay with her until 3am. The following morning she is told by a nurse that “it had been a very close run thing and [that she] had been very lucky to survive it”.
Later that morning, before any assessment, J tries to leave the hospital to run away with the intention of going to kill herself. She is brought back in by hospital security. At no point does J say that she wants to be admitted to mental health hospital. It is my firm belief she wasn’t, in some way, trying to manipulate or “play the system” and that every aspect of her crisis was genuine.
Eventually, after a bed search over the phone, she is admitted to Bosworth Ward at the Bradgate Mental Health Unit on Saturday 19th July. She is told by hospital staff that she is “lucky” to have been given a bed locally.
In light of the fact that J had recently left hospital and was struggling to cope at home, I am dismayed at the attitude of NW in her assessment of J’s risk to herself. The fact that we were finding ourselves in these situations seemed to be used against J, as if this was a type of stock behaviour designed to provoke a certain type of response in professionals, when in fact she was a genuine danger to herself, and that my (and the police’s) efforts to her keep safe up to that point were meaningless. The fact that it was I who was phoning the police and not J, seemed to mean nothing. The fact that I had begged J to co-operate and come with me to the Urgent Care Centre or to let the Police take her back to the station without her struggling, bore no evidence to your staff. Even if she was merely “crying for help” I still believe that Ms.NW’s assessment was grossly negligent, because my partner would be dead now. This was after trying to reach an identified hotspot twice, declaring an alternative method (overdose by pills) and being allowed access to the means to doing that (taken home where her medication was). Had J been taken straight to a place of safety and admitted immediately to a hospital for treatment, many of the events of Friday 18th July could have been avoided. I believe that by belittling J’s views, dismissing her difficulties and saying specifically triggering things, that NW turned J’s complicated plan of suicide (the motorway bridge - a specific location, outside of Loughborough) into a more easily accessible plan – her pills at home (for fear of police cells, or worse, people thinking badly of her).
I am especially saddened by all this because, until recently I ran two mental health drop-ins in Loughborough (Age UK L,S&R for LCC) and we advised service users of the drop-ins to do all of the things that J did when in they were crisis (within the differing contexts of care plans where present). I was appalled by the attitude of Ms.NW, especially in a role where she is assessing people who the police have already deemed as unsafe to themselves. At least on the previous night J had felt she had been taken seriously by mental health worker, V_, despite her failure to also affect any real change or to keep J safe from herself.
Yours faithfully
(my name)
Partner, and informal carer for J.




















{kind=link}